If you ask a hospital CFO what physician burnout costs their organization, you'll usually get an answer measured in morale. Sometimes a reference to a recent staff survey that showed declining satisfaction scores. Rarely do you get a number.
The problem reveals itself when you actually run the math — recruiting fees, locum coverage, onboarding time, lost visit revenue, malpractice exposure during the transition period. According to Christine Sinsky, MD, vice president of professional satisfaction at the American Medical Association, replacing a single physician costs anywhere between $500,000 and $1,000,000. AMN Healthcare's research puts the figure similarly, noting that combined search costs and lost revenue can drive the total cost of replacing one physician well beyond $500,000. AMN Healthcare For surgical specialists, the number climbs higher still.
In most cases, the driver behind most of those departures isn't compensation or management, but documentation. And most healthcare organizations are still treating it as a morale problem rather than the economic one it actually is.
The Documentation Load Nobody Talks About in Board Meetings
The research on this is consistent, and has been for years. According to a landmark study published in JAMA Network Open, physicians spend approximately 1 to 2 hours on documentation for every 1 hour of direct patient care. In some specialties such as internal medicine, family practice, psychiatry it skews even higher.
That means that in a standard eight-hour clinical day, a physician might be spending three to four hours generating notes, completing prior authorizations, updating referral records, coding encounters for billing, and fighting with EHR systems that were designed by people who have never practiced medicine.

Multiply 3-4 hours per physician across a department of even a health network. The number gets uncomfortable very quickly.
What makes it worse is that a meaningful portion of this documentation is happening after hours. Physicians log back in at 9pm to finish the notes from their afternoon clinic. They complete discharge summaries on weekends. The term clinicians use for this is "pajama time", a phrase that sounds almost charming until you understand what it signals about the structural failure underneath it.
Burnout Is a Lagging Indicator
Burnout accumulates gradually, and documentation burden is one of its most reliable accelerants. Here's how the pattern typically unfolds in a clinical environment:
- Documentation starts eating into patient time. A physician scheduled for 20-minute appointments begins spending 5 of those minutes typing instead of examining or listening. Clinical presence declines, and patient satisfaction scores follow.
- After-hours charting becomes routine. What started as occasional catch-up becomes structural. The physician's personal time is now a de facto extension of the documentation workload.
- The physician begins reducing clinical hours. To protect personal time, they cut their schedule with fewer patients per day and shorter weeks. This directly impacts throughput and revenue.
- The physician begins exploring alternatives. They may entail locum work, administrative roles, early retirement, or a move to a cash-pay practice where documentation requirements are simpler.
- The departure. And suddenly the organization is looking at an open position, a search process, and a bill that could easily exceed $750,000 before the replacement physician is seeing patients independently.
By the time an exit interview confirms "burnout" as the reason, the documentation problem that drove it has been accumulating for two or three years. The organization reacts to the departure. The documentation burden that caused it remains unchanged for the next physician in that seat.
The Real Cost Breakdown: Running the Numbers
Below is a conservative estimate of what a single physician departure costs a mid-sized health network, assuming a primary care or internal medicine profile.
| Cost category | Estimated range |
| Executive search / recruitment fee (20–30% of first-year salary) | $50,000 – $90,000 |
| Locum tenens coverage (per week, avg. 12–20 weeks) | $120,000 – $200,000 |
| Lost visit revenue during vacancy (est. 800–1,200 visits/month) | $80,000 – $150,000 |
| Onboarding and credentialing time (new hire at partial capacity, 3–6 months) | $60,000 – $120,000 |
| Training, orientation, and systems integration | $15,000 – $30,000 |
| Productivity ramp-up gap (months 1–6 at 60–70% of full capacity) | $40,000 – $80,000 |
| Total estimated cost per departure | $365,000 – $670,000 |
Surgical specialists, subspecialists, and senior clinicians with established patient panels will sit at the higher end or above. Academic positions with research responsibilities often carry additional transition costs.
These figures do not include the downstream impact on care continuity such as patients rescheduling, care gaps forming, specialist referrals delayed. The true organizational cost is higher, but the clinical cost is harder to quantify.
Now consider that physician turnover rates in many healthcare systems currently run between 10% and 20% annually, with burnout cited as the primary or contributing factor in most voluntary departures. For a health network with 200 physicians, that's 20 to 40 departures per year at costs ranging from $7M to $25M or more.
Most of those organizations are managing this as a retention challenge. Very few are identifying the documentation workload as the operational lever that's most directly addressable.
Why Most Documentation Tools Don't Actually Solve the Problem
Here's where I want to be direct about something: the market is full of solutions that claim to address this, and most of them don't.
Generic speech-to-text tools, he kind that transcribe audio and produce a raw text block, do exist. Some clinicians use them aimed to reduce typing. They do not reduce documentation burden in any meaningful structural sense, because the physician still has to turn that raw transcript into a structured, compliant clinical note. The administrative work just shifts from keyboard entry to transcript editing.
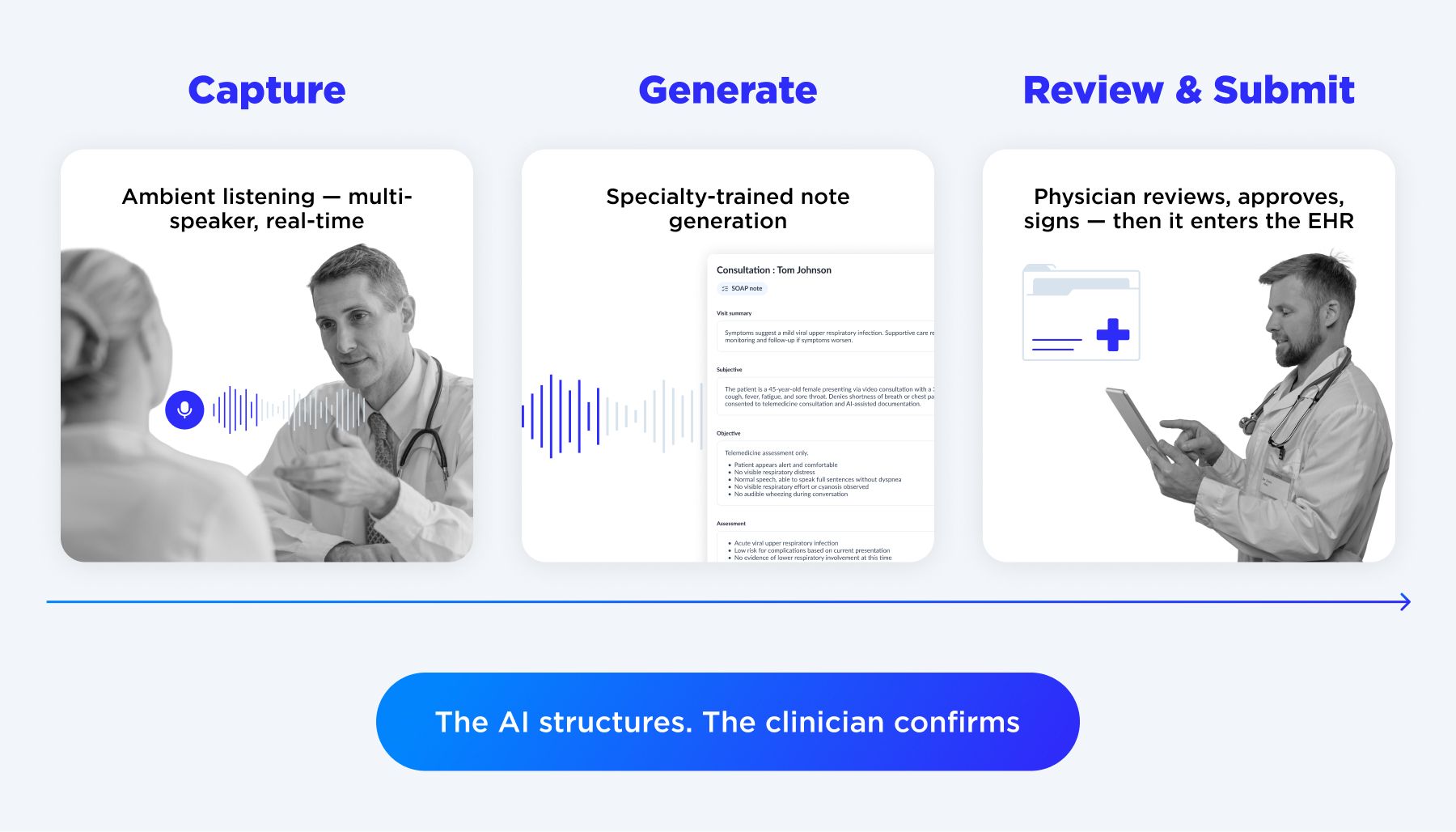
What actually works is a different category entirely: ambient clinical intelligence that listens to the patient-physician interaction, understands the clinical context (not just the words), generates a structured note in real time, and routes that note to the physician for review and approval before it ever enters the EHR. The physician doesn't touch a keyboard during the encounter. They spend five minutes reviewing and signing at the end, rather than forty minutes documenting from memory.

The difference isn't incremental. In deployments we've run through Medical Scribe AI software, clinical documentation time drops by 60–65% on average. Physicians get their evenings back. After-hours charting essentially disappears for the physicians in the program.
What MedScribeAI Actually Does
MedScribeAI is OTAKOYI's custom-built ambient documentation platform, designed specifically for clinical environments where generic tools fall short.
During a patient encounter, it listens using noise-resistant, multi-speaker audio models, recognizes clinical context like symptoms, diagnoses, medications, vitals and generates a structured note in real time, formatted to your specialty and templates. Oncology reads differently from psychiatry. Primary care notes look nothing like surgical summaries. The system is trained to understand the difference.
After the encounter, the note routes to the physician for review. A built-in change tracking and versioning layer means every edit is logged. Nothing enters the EHR without explicit sign-off.
On the integration side, MedScribeAI connects to any EHR via HL7/FHIR , including legacy and regional systems, with bi-directional data sync and custom field mapping. Data stays within your chosen environment: on-premise, private cloud, or hybrid, with full compliance with HIPAA, GDPR, and regional equivalents built into the architecture rather than bolted on.
For medical leadership, a live analytics dashboard tracks documentation time saved per clinician, error rates, template performance, and system-wide adoption, giving operations a measurable view of ROI from day one.
The Compliance Dimension Nobody Wants to Talk About
There's another cost layer that rarely appears in retention discussions – documentation quality as a compliance and revenue risk. Incomplete or inconsistent clinical documentation creates three distinct exposure points:
- Claim denials. Payers audit for documentation quality. If a clinical note doesn't adequately support the complexity of the encounter being billed, the claim gets downgraded or denied. This happens silently, at scale, across hundreds or thousands of encounters per month. The revenue impact is significant and largely invisible in most organizations' financial reporting.
- Audit risk. A documentation pattern that looks like upcoding, even when the clinical encounters genuinely justify the billing level, becomes a liability in an audit context. The asymmetry here matters: the clinical work was done, but the documentation didn't capture it.
- Care continuity failures. When a note is incomplete, the next clinician who sees that patient is working from incomplete information. This produces redundant tests, missed context, and in the worst cases, clinical errors. The medico-legal exposure here is real and grows proportionally with patient volume.
None of these risks are hypothetical. They're active in every health network that relies on manual documentation, and they compound over time.
What a documentation-first approach to retention actually looks like
I want to give you a concrete picture of what the alternative looks like, because "AI-assisted documentation" still sounds abstract to a lot of medical executives.
In a typical deployment, the implementation follows a staged approach that doesn't disrupt existing clinical workflows:
Stage 1 — Clinical AI Readiness Audit (3 weeks).
We analyze the documentation workflow across selected departments and deliver a compliance gap assessment, a MedScribeAI fit report, a financial impact model connecting your documentation burden to physician retention risk, and a phased deployment roadmap with Week 1 go-live scope defined. Most organizations find this reframes the conversation internally: from a morale problem to an economics one.
Stage 2 — MedScribeAI Deployment (16–20 weeks).
You receive a fully configured and integrated ambient scribe platform — EMR-connected via FHIR/HL7, compliant with regional privacy requirements, staff trained, and a real-time analytics dashboard live from day one. Rollout is specialty-by-specialty, with a clinical champion per department, and physician adoption measured against the Stage 1 baseline. Every note requires explicit physician review and approval before it enters the record.
Stage 3 — Scale Team Retainer (3-month minimum).
An embedded AI Product Engineer with healthcare domain specialization handles ongoing specialty expansion, additional EMR integrations, compliance monitoring, and monthly analytics reporting to medical leadership.
Every note generated by the AI requires explicit physician review and approval before it enters the EHR. The AI never writes to the record unsupervised. Clinicians retain full control and full accountability — the system supports, it does not replace.

Book a Clinical AI Readiness Audit
CONTACT USThe Cost of Doing Nothing
I want to end on a point that doesn't get made directly enough in most conversations about clinical AI.
Continuing to rely on manual documentation, hoping that physicians will adapt, treating burnout as an inevitable feature of clinical work has a price. It's just a price that's distributed across many budget lines and rarely aggregated in a way that makes the decision obvious.
Across a year, that price looks something like this for a 100-physician network running 15% annual physician turnover:
- 15 physician departures at $500K average cost: $7.5M
- Revenue lost to documentation-driven throughput constraints (conservative 10% reduction): $3–6M
- Claim denials and coding downgrades from inconsistent documentation: $500K–$2M
- Total estimated annual cost of inaction: $11M–$15M+
Compare that to the cost of deploying an ambient documentation platform across that same network. The question isn't whether clinical documentation automation makes financial sense. For organizations operating at any meaningful scale, it does — clearly, demonstrably, and increasingly urgently as both regulatory requirements and physician supply constraints tighten.
What to Do Next
If you're a medical executive reading this and the numbers in the cost breakdown feel familiar — if physician turnover, documentation backlogs, and after-hours charting are active conversations in your organization — the most useful next step isn't a product demo.
It's an honest assessment of what your current documentation workflow is actually costing.
That's exactly what our Clinical AI Readiness Audit is designed to surface: a documentation workflow analysis across selected departments, a compliance gap assessment, and a financial model connecting your specific documentation burden to physician retention risk. The output includes a phased deployment roadmap built around your existing infrastructure.
It takes three weeks, and costs a fraction of a single physician replacement. And for most organizations that go through it, the output reframes the conversation from "should we do this" to "why haven't we started."
At OTAKOYI, we build ambient AI documentation platforms for healthcare organizations that want to reduce clinician burnout, improve documentation quality, and integrate AI safely into existing clinical workflows, without replacing the physician at the center of every decision.